Innovators of 3D-printed activator appliance, Dr. Akshay Parmar and Dr. Krishnakumar Jaju, say that it can be efficient and effective in improving the sagittal molar relationship for the treatment of Class II skeletal malocclusion.
Why did you create it?
Class II malocclusion presents a major and common challenge to orthodontists. Class II discrepancies with mandibular deficiency during active growth are usually treated using myofunctional appliances. In patients, who have not yet crossed the adolescent growth spurt, removable functional appliances such as Activator, Bionator, Twin Block, and Frankel may be used.
The activator appliance which was designed by Andresen and Haupl (1908), has been proved a popular and clinically successful appliance. The complexity in the lab procedure and ill-fitting of the appliance made us think of fabricating the activator by 3D printing.
What problem does it solve?
The warpage of the wax during the transportation of the bite is avoided. The conventional method of impression making is eliminated as the impressions are made using an intraoral scanner. Chairside time consumed for constructing the bite is reduced. Human errors, such as porosity which is seen in the appliance while fabricating using the conventional method, are eliminated. It can be easily refabricated if lost or damaged. There is a precise fit and enhanced accuracy of the appliance compared to the conventionally fabricated appliance. Finishing and polishing time is reduced.
How did you test it?
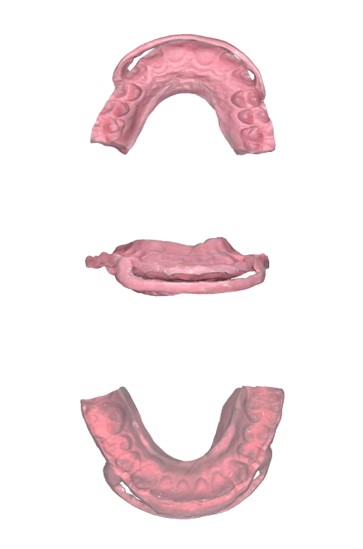
A patient was selected with a Class II skeletal discrepancy with a deficient mandible. Two ice cream sticks were used to make notches for the desired occlusion. Upper and lower arches were scanned completely using an intra-oral scanner. The patient was then asked to position the mandible forward in the desired occlusion. The notches on the ice cream sticks were used as guidance to bite between the upper and lower incisors to help stabilize the desired occlusion. A complete bite scanning was performed using an intra-oral scanner in the desired occlusion. 3D reference models were then printed in the desired occlusion using a resin material.
The appliance was designed virtually on the upper and lower models. A prototype of the activator was then fabricated using the same 3D printer. The prototype was used to check for the fit and finish on previously printed reference models. The activator was printed using a 3D printer with a biocompatible resin material.
Antero-posterior correction of buccal segments was achieved after eigth months of full-time wear. In occlusion, there were substantial lateral open bites and minimal functional occlusal contacts. Hence we concluded that a 3D-printed activator appliance can be efficient and effective in improving the sagittal molar relationship for the treatment of Class II skeletal malocclusion.
Current status and future plans
We have already completed the evaluation of this 3D-printed activator and have received promising data. We hope to achieve positive results which can help us in promoting our 3D-printed activator for routine use thus improving the overall efficiency of Class II discrepancies with mandibular deficiency.
DAMMAM, Saudi Arabia: The method of denture fabrication and material used are relevant to longevity, strength and occlusal wear resistance. 3D-printing ...
MOSCOW, Russia: Researchers from Austria, Germany and Russia have collaborated in successfully using lithography-based ceramic manufacturing (LCM), a form ...
Smile Designing doesn’t always have to be about elaborate, extensive and invasive procedures but just sometimes routine procedures done with adherence to ...
COLOGNE, Germany: Today, Dental Tribune International hosted the founding meeting of the International Academy for Dental 3D Printing (iad3Dp). The goal of ...
EDMONTON, Canada: A team of researchers at the University of Alberta has secured funding to develop a 3D ultrasound device that would allow dentists to ...
XI'AN, China: In a independent surgery, a robot has placed two 3-D-printed implants into a patient’s mouth. The successful procedure can be one of the ...
Education
Live webinar Fri. 7 August 2026 2:30 am IST (New Delhi)
Digital tools are reshaping diagnosis, treatment planning, restorative workflows and implant dentistry—but technology creates clinical value only when ...
Tooth decay remains the most widespread chronic health condition globally, affecting billions of people. While cavities are largely preventable and ...
MUMBAI, India: Can clinicians identify patients at higher risk of implant complications before surgery? Can understanding the patient’s immune response ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CELive webinar
Cat EdneyRegister now1CELive webinar
 Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE
Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE











































To post a reply please login or register