On 7 May 2021, the UK flagged the Indian variant B. 1. 617.2. as a variant of concern (VOC) from its earlier designation of only variant of interest (VOI).
This is a series of updates by Dr. Rohan Bandi, a prosthodontist from Mumbai, on the emerging updates on B.1.617.2 the Indian variant of SARS-CoV-2.
In December 2020, different scientific departments of India came together to set up the Indian SARS-CoV-2 Consortium on Genomics (INSACOG), which aims to identify variants of concern through sequencing of the SARS-CoV-2 RNA.
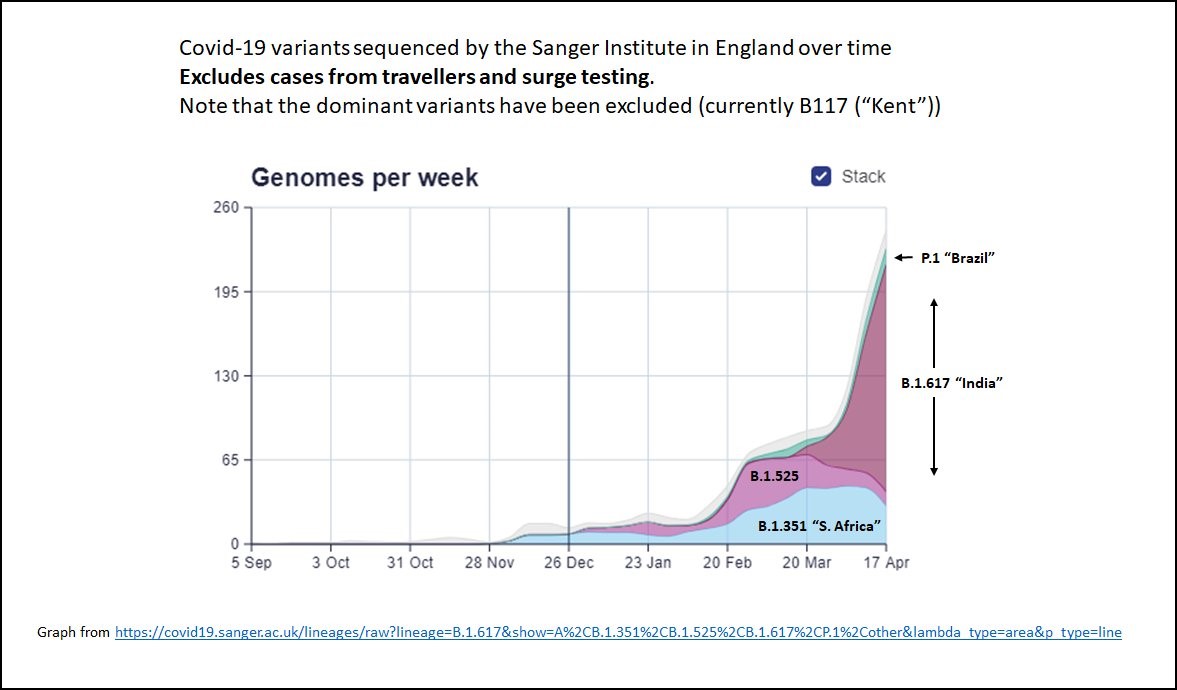
In March 2021, INSACOG identified a variant that was not reported elsewhere globally (although a similar variant was also discovered in October 2020). The variant had two changes in the string of the SARS-CoV-2 RNA sequence, which are thought to make it a variant that needs close monitoring. This variant of the SARS-CoV-2, which arose in India, is now termed as the B.1.617. The term has come into use according to the naming criteria of this subtype of the virus, that is, its lineage (earlier had a misnomer of "double mutant"). [1]
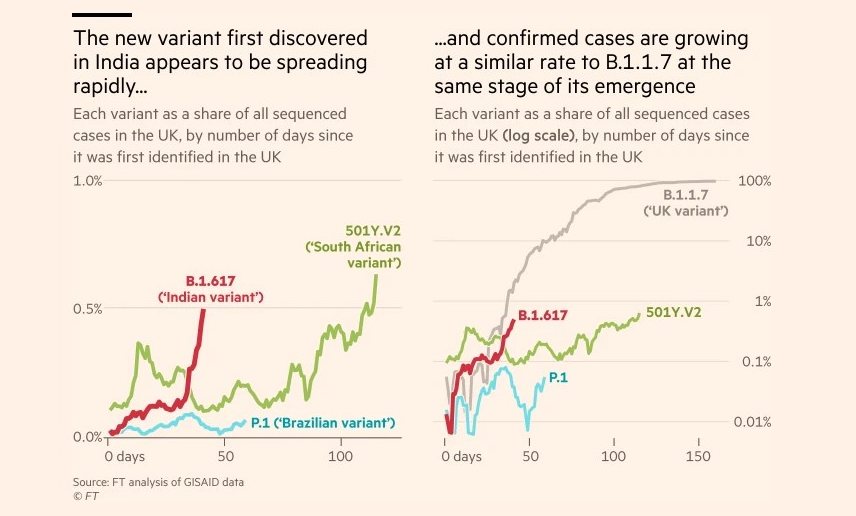
In the last two and half months, the B.1.617 lineage has become prevalent in almost all states of India and 19 countries globally, and it is only spreading to more countries.
The UK, on 7 May 2021, flagged the Indian variant B. 1. 617.2. as a Variant of concern (VOC) from its earlier designation of variant of interest (VOI ).
The new designation came in as multiple clusters of cases of the Indian variant (B. 1. 617) were detected in many pockets across the UK. Many of these cases had no travel history to India, so the possibility of the virus having community spread and increased transmissibility is very real.
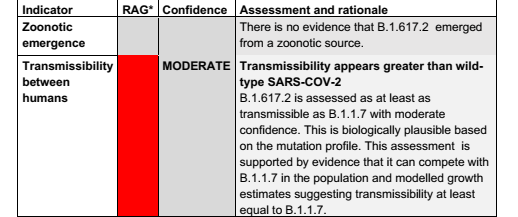
The lineage has been assigned a VOC clearly because of increased transmission, and as per assessment, it is AT LEAST as much transmissible as B.1.1.7 (Kent) variant.
The lineage has been assigned a VoC clearly because of increased transmission and as per assessment, it is AT LEAST as much transmissible as B.1.1.7 (Kent) variant pic.twitter.com/MX3Acjwo8n
Dr. Deepti Gurdasani, a clinical epidemiologist and senior lecturer at the Queen Mary University of London, said the variant was "increasing very rapidly" and that "at the current doubling rate it could easily become dominant in London by the end of May or early June."
One such cluster where 15 cases of B.1.617.2 were found in one London care home where residents had their second doses of the Oxford/AstraZeneca vaccine in the week before the outbreak.
Four of the cases were hospitalized with a non-severe illness, and there were no deaths. [2]
Children from 5 schools among Israel's 41 cases of Indian COVID strain B.1.617, in individuals without travel history, indicating community spread. 10% of the infected were fully vaccinated. [3]
Keeping it out will not be easy, says Tom Wenseleers (@TWenseleers), Professor of Biology and biostatistics at
KU_Leuven Belgium.
Twenty out of 43 Indian students arrived with a B.1.617.2 infection after a negative Rt-PCR test before departure and another negative antigen test in Charles de Gaulle airport in Paris. Eight out of 20 were vaccinated.
(10/11) Keeping it out won't be easy. In BE, we just had 20/43 Indian students arriving with a B.1.617.2 infection, after a neg PCR test prior to departure and another neg Ag test in Charles de Gaulle airport in Paris. 8 out of 20 were vaccinated. https://t.co/bYehjTHCLM
Editorial note: With inputs from Dr Ameet Revankar (MDS, Orthodontics), SDM College of Dental Sciences & Hospital, Sattur, Dharwad. A list of references is available from the publisher.
Several media reports have come up with scary headlines that the new SARS-CoV-2 variants are fooling the RT-PCR test, which is considered the gold standard ...
In this article, we analyze four recent articles published in Aug-Sept 2020 on the genetic diversity of SARS-CoV-2 and the potential therapeutic targets ...
LEIPZIG, Germany: Researchers in India have found that scientific literature supports salivary diagnostics for SARS-CoV-2 infection as an alternative to ...
LEIPZIG, Germany: UK health authorities have administered the first doses of the SARS-CoV-2 vaccine developed by Pfizer and BioNTech, and public health ...
The World Health Organization (WHO) updated its communication on the airborne transmission of SARS-CoV-2 on 30 April 2021.
This article summarizes their ...
LEIPZIG, Germany: New variants of the SARS-CoV-2 virus that emerged in the UK and South Africa in 2020 show higher transmissibility. And whereas they are ...
BRISTOL, UK: The largest study to date specifically measuring aerosol generation in dental settings found that many common procedures produced negligible ...
Tooth decay remains the most widespread chronic health condition globally, affecting billions of people. While cavities are largely preventable and ...
MUMBAI, India: Can clinicians identify patients at higher risk of implant complications before surgery? Can understanding the patient’s immune response ...
Implant dentistry has evolved significantly through advances in implant design, surface technology and digital workflows. However, the process of osteotomy ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE










































To post a reply please login or register