The World Health Organization (WHO) has been in the limelight for many wrong reasons too, since the beginning of SARS-CoV 2. The latest controversy has been about a statement that said 'infection spread from asymptomatic individuals is very rare,' which drew criticism from epidemiologists across the world. Read the full story.
The latest to the tally of confusing statements issued by the WHO is the one made by Maria Van Kerkhove, an epidemiologist and WHO’s the technical lead on the coronavirus pandemic who said on Monday the 8th of June that the infection spread from asymptomatic individuals is very rare, and that many countries undertaking contact tracing had identified asymptomatic cases, but were not finding they caused further spread of the virus. “It is very rare,” she said. (1)
But soon her comments went viral and created a lot of confusion among health professionals and the common public. Experts of different field expressed mixed reaction to the new WHO guidelines. Many said they would like to go through the references on which the statements were made. (1)
These comments were very different or contrary to the previous views and guidelines that asymptomatic carriers account for majority of the spread of the virus in people. (2,3)
Fearing flak and criticism, Van Kerkhove acknowledged on 9th June 2020 that her use of the phrase “very rare” had been a miscommunication. She said she had based that phrasing on findings from a small number of studies that followed asymptomatic cases and tracked how many of their contacts became infected. She said she did not mean to imply that “asymptomatic transmission globally” was happening rarely because that has not been determined yet. (4)
Then what should we imply? Should we read between the two contrary lines? Was it just bad diction on WHO's part? Should the new studies on which her comments were based, be considered game-changers?
We decided to go through the actual reference articles to have a better idea of what the studies implied. The WHO released interim guidance on the use of masks in the context of COVID-19. (5) Before we go into the details of the guidance, let's just update ourselves with a few terms.
Asymptomatic: people who are infected but never go on to develop symptoms
Pre-symptomatic: people who are infected but have not yet developed symptoms
Symptomatic: people who are infected and showing symptoms. (6)
Natalie E. Dean, PhD Assistant Professor of Biostatistics at UF and HarvardBiostats PhD tweeted –
My take on @WHO press conference on asymptomatic transmission - sounds like a misunderstanding. WHO is drawing a distinction between transmission from people who are fully asymptomatic (never develop symptoms) and pre-symptomatic (haven’t developed symptoms yet). 1/3
— Natalie E. Dean, PhD (@nataliexdean) June 8, 2020
WHO interim guidance on the use of masks and Transmission in the context of COVID-19
Coming back to the guidance, it says - Current evidence suggests that most transmission of COVID-19 is occurring from symptomatic people to others in close contact, when not wearing appropriate PPE. (5)
Prolonged RNA shedding, however, does not necessarily mean continued infectiousness. Transmissibility of the virus depends on the amount of viable virus being shed by a person, whether or not they are coughing and expelling more droplets, the type of contact they have with others, and what IPC measures are in place.
Among symptomatic patients, viral RNA can be detected in samples weeks after the onset of illness, but the viable virus was not found after day 8 post-onset of symptoms for mild patients, though this may be longer for severely ill patients. (5)
Faheem Younus; MD, Chief of Infectious Diseases, University of Maryland Upper Chesapeake Health explains this
COVID Tip:
Early in the disease, a patient may have no symptoms and the PCR test may be (-) but the patient IS CONTAGIOUS.
10-11 days later, the patient may still have cough and test may still be +, but the patient is NOT CONTAGIOUS.
The guidance further says - There is also the possibility of transmission from people who are infected and shedding virus but have not yet developed symptoms; this is called pre-symptomatic transmission. The incubation period for COVID-19, which is the time between exposure to the virus and symptom onset, is on average 5-6 days but can be as long as 14 days.
Pre-symptomatic transmission is defined as the transmission of the COVID-19 virus from someone infected and shedding virus but who has not yet developed symptoms. People who develop symptoms appear to have higher viral loads on or just prior to the day of symptom onset, relative to later on in their infection. (5)
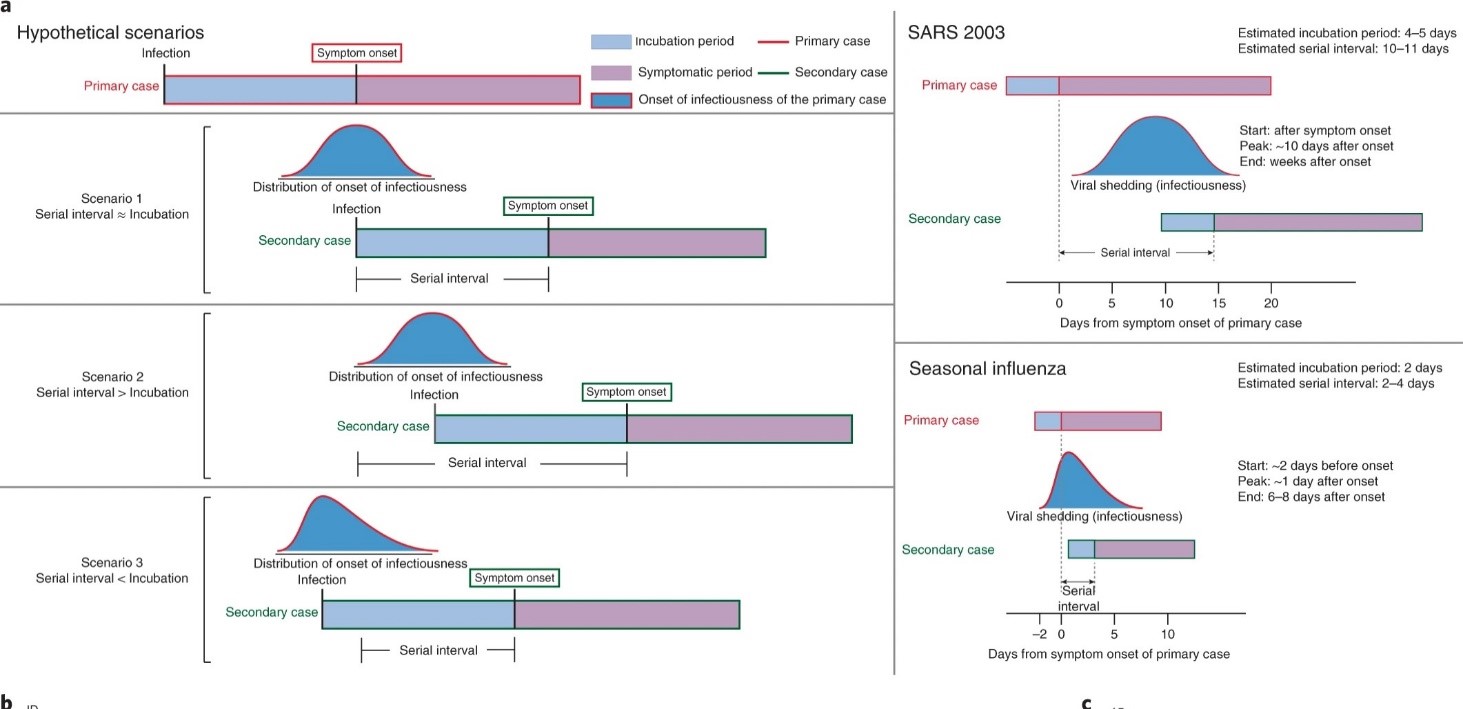
The same as illustrated in this study by Xi He, Eric Lau et al (9) showed that the highest viral load in throat swabs at the time of symptom onset, and inferred that infectiousness peaked on or before symptom onset. (FIG:1)
Fig 1: infectiousness peaked on or before symptom onset
Infectiousness profile of SARS CoV-2 may more closely resemble that of influenza than of SARS.
SARS (severe acute respiratory syndrome) was notable because infectiousness increased around 7–10 days after symptom onset. Onward transmission can be substantially reduced by containment measures such as isolation and quarantine. In contrast, influenza is characterized by increased infectiousness shortly around or even before symptom onset.
The WHO guidance further states - some people infected with the COVID-19 virus do not ever develop any symptoms, although they can shed virus which may then be transmitted to others.
One recent systematic review found that the proportion of asymptomatic cases ranged from 6% to 41%, with a pooled estimate of 16% (10)
Comprehensive studies on transmission from asymptomatic individuals are difficult to conduct, but the available evidence from contact tracing reported by the Member States suggests that asymptomatically-infected individuals are much less likely to transmit the virus than those who develop symptoms. (5)
Among the available published studies, the chances of an asymptomatic positive case infecting another person with SARS-CoV2 are in the range of 0 % i.e. Zero transmission for one study (11), 6.4% for one study (12), but this study counted pre-symptomatic and asymptomatic together while reporting and 14% in another study (13).
The available data, to date, on onward infection from cases without symptoms comes from a limited number of studies with small samples that are subject to possible recall bias and for which fomite transmission cannot be ruled out. (5)
What specifically interested us were these 2 recent articles.
1. A systematic review by Byambasuren, O. Cardona et al (10) which is in pre-print stage and available on MedRxiv.
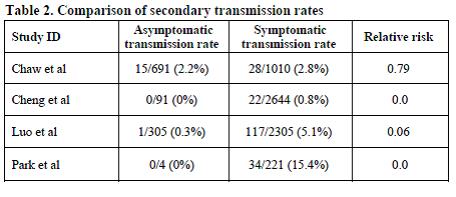
In this article 4 studies reported data on secondary infection transmission from asymptomatic cases (Table 1). The asymptomatic transmission rates ranged from none to 2.2%, whereas symptomatic cases transmission rates ranged between 0.8-15.4%
Table 1. Comparison of secondary transmission rates
Estimates of the proportion of asymptomatic cases and their transmission rates suggest that asymptomatic spread is unlikely to be a major driver of clusters or community transmission of infection, but the extent for pre-symptomatic and minor symptomatic transmission remains unknown. (10)
Their recommendations for future research also include improved clearer reporting of methods, sampling frames, case definition of asymptomatic, extent of contact tracing, duration of follow-up periods, presentation of the age distribution of asymptomatic cases and separation of pre-symptomatic and mild cases from asymptomatic cases in result tables.
Their estimates of the prevalence of asymptomatic COVID-19 cases and asymptomatic transmission rates are lower than many highly publicized studies, but still sufficient to warrant policy attention.
They also suggested that further robust epidemiological evidence is urgently needed, including in sub-populations such as children, to better understand the importance of asymptomatic cases for driving spread of the pandemic. (10)
2. A cohort study by Luo, L., Liu, D et al (14) in pre-print available on MedRxiv shows that among different modes of contact, household contacts were the most dangerous in catching with infection of COVID-19, with an incidence of 10.2%.
As the increase of age for close contacts and severity of source cases, the incidence of COVID-19 presented an increasing trend from 1.8% (0-17 years) to 4.2% (60 or over years), and from 0.33% for asymptomatic, 3.3% for mild, to 6.2% for severe and critical source cases, respectively.
The manifestation of expectoration in source cases was also highly associated with an increased risk of infection in their close contacts (13.6%).
Secondary cases were in general clinically milder and were less likely to have common symptoms than those of source cases.
They concluded by saying that, the proportion of asymptomatic and mild infections account for almost half of the confirmed cases among close contacts. Also, asymptomatic or mild cases combined represent about 40% to 50% of all infections.
The household contacts were the main transmission mode, and clinically more severe cases were more likely to pass the infection to their close contacts.
Generally, the secondary cases were clinically milder than those of source cases.
They inferred that the results provided the evidentiary foundation for evaluating control measures and guiding the global response. Given the current evidence, as asymptomatic cases have limited transmission capacity, the primary surveillance and control measures should focus on symptomatic contacts.
Limitation of the above 2 articles is that they are yet in pre-print and yet to be peer-reviewed.
So, an error in diction by Maria Van Kerkhove?
Well according to our detailed analysis of the references cited by WHO and the 2 recent studies published, it appears to be neither an error in diction nor confusion.
But rather new learning in the infectivity, transmission and prevalence of the SARS-CoV 2 virus. Her comments were based on the results published in the above two studies.
The above studies do show that truly asymptomatic and mildly symptomatic cases have limited transmission capacity and control measures should focus on symptomatic contacts.
Now whether it can be termed “very rare” is subjective. The Word ‘rare’ any which ways is subjective. Doesn’t imply what the prevalence is.
The probable reason why W.H.O. had to issue a clarification on Tuesday the 9th of June 2020 saying there was “miscommunication” was because still further studies are needed to verify these results and until further studies supporting the above results are published, policy decisions and global response guidelines cannot be made.
Do the studies warrant any change for dental protocols?
Currently, with limited research and limited good peer-reviewed studies published, it would be too early to warrant any changes in our COVID protocols. At best the only thing we can say is that the risk perceived to us in contacting the virus is less than the earlier perceived if proper guidelines are followed.
However, discussing the evidence on risks of Aerosol Generating Procedure (AGP) in asymptomatic patients is beyond the scope of this article.
He X, Lau EHY, Wu P, Deng X, Wang J, Hao X, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26(5):672-5.
Byambasuren, O., Cardona, M., Bell, K., Clark, J., McLaws, M.-L., Glasziou, P., 2020. Estimating the extent of true asymptomatic COVID-19 and its potential for community transmission: systematic review and meta-analysis (preprint). Infectious Diseases (except HIV/AIDS). MedRxiv. [preprint].(https://www.medrxiv.org/content/10.1101/2020.05.10.20097543v1, accessed 4 June 2020) https://www.medrxiv.org/content/10.1101/2020.05.10.20097543v2
Cheng HY, Jian SW, Liu DP, Ng TC, Huang WT, Lin HH, et al. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern Med. 2020.
Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. Presymptomatic Transmission of SARS-CoV-2 - Singapore, January 23-March 16, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(14):411-5.
Wang Y, Tong J, Qin Y, Xie T, Li J, Li J, et al. Characterization of an asymptomatic cohort of SARS-COV-2 infected individuals outside of Wuhan, China. Clin Infect Dis. 2020.
Luo, L., Liu, D., Liao, X., Wu, X., Jing, Q., Zheng, J., et al., 2020. Modes of contact and risk of transmission in COVID-19 among close contacts (preprint). MedRxiv. [preprint].(https://www.medrxiv.org/content/10.1101/2020.03.24.20042606v1, accessed 4 June 2020)
Addendum:
Another study published on 12th June 2020 in the New England Journal of Medicine by Aki Sakurai et al on the outbreak of COVID 19 on the cruise ship 'Diamond Princess' shows some interesting evidence. Two salient points from the study are
1) The percentage of asymptotic infected people could be as high as 58% although the line between asymptomatic and very mildly asymptotic is ill-defined and individual bias is always present as what they perceive as no symptoms and mild symptoms.
2) PCR test turned negative in 48% of individuals by day 8 and 90% by day 15. However, the duration of infectivity and PCR remaining positive increases with age.
Whether the spread of infection among 712 out of 3711 passengers on board the ship occurred from asymptotic, pre-symptomatic, symptomatic or all 3 could not be inferred from this study. Click here to read this study
Author:
Dr. Rohan Bandi, MDS in Prosthodontics from Manipal University, was previously attached to Wockhardt Hospital, Mumbai central as a chief consulting dentist. He is currently the director and owner at “World Smiles, dental center” and a consultant at several clinics in Mumbai. His main area of interest is esthetic dentistry in which he has done a credible amount of research and treated numerous cases nationally as well as internationally. Health Care Research is his another area of interest.
The possible benefits by which one can use mobile applications (apps) for contact tracking in managing the COVID-19 pandemic have been discovered. Various ...
Dental Tribune South Asia has launched COVIDEAS - an initiative to encourage innovative thought processes and bring innovative ideas to the attention of ...
The new CDC estimates for the severity, complications and deaths of COVID-19 bring down the numbers much lower making the overall scenario very optimistic. ...
Mansoor Ali, a research analyst and veteran in the air treatment products industry, speaks about the role of relative humidity in controlling the spread of ...
CHICAGO, Ill., USA: According to a new policy from the American Dental Association, point-of-care testing to screen patients for chronic diseases and other ...
This guest editorial by Dr Sanjiv Hyoju talks about a possible connection between a diet-induced disturbance in the gut microbiome equilibrium and its ...
Dr Ashwini Bhangale (BDS) summarizes the latest updates on the use of masks - from the World Health Organization (WHO), released on 1 Dec 2020 and the ...
The recent 'Times Fact India Outbreak Report' suggests that around 22 May 2020 India could see the number of coronavirus cases surge up to 75,000. Experts ...
Education
Live webinar Tue. 4 August 2026 5:30 am IST (New Delhi)
Tooth decay remains the most widespread chronic health condition globally, affecting billions of people. While cavities are largely preventable and ...
MUMBAI, India: Can clinicians identify patients at higher risk of implant complications before surgery? Can understanding the patient’s immune response ...
Implant dentistry has evolved significantly through advances in implant design, surface technology and digital workflows. However, the process of osteotomy ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE






















 on Covid-19 spread & SARS-CoV-2 testing: Relevant to dentists")

 from WHO's 3.4% (CFR)")




 updates from WHO and CDC on the use of masks in the context of COVID-19")















Good Work. Dr.Rohan Bandi
Very informative article!
Fantastic.very informative