COVID-19 is having an unprecedented impact on the global economy, including that of the dental industry. Most dental clinics are shut and a few are offering only the emergency services. Dr Bhavdeep Ahuja will analyse “the rising costs in the oral health care services and how to reboot and restart the dental clinics” in his 5 part series. “Changing Life Scenario in the Post COVID-19 Era” – is the first article of the series.
(Author Disclaimer: This article of mine is targeted at small to medium level dental practitioners and new practitioners who deal in a limited level OPD and have small to medium-sized premises. No disrespect, whatsoever to those who are having big spacious interiors, jam-packed OPD’s and big numbers (financial) associated with their name. I would like to re-iterate here that the distinguishing factor is the number of patients and size of the practice and not the skill set of any individual which can be highly inequitable. The only reason for dishing out this disclaimer is that highly successful running dental clinics won’t find the content of the article identifiable and suitable for adaptation in their enormous practices, but, if willing to, can read on and send your feedback to me)
ABSTRACT
The most prudent upcoming challenge in the post-COVID-19 era is the increase in the cost of oral health services which can limit the patient access to health care as limited resources lead to rationing and delaying and denial of care to people in need. We are in the Lockdown almost all over the world due to a pandemic called ‘Coronavirus’ aka the COVID-19. Of course, the human race has been known to overcome all such challenges in the past. One aspect is, however, getting absolutely clear; practising Dentistry in future (Post-COVID-19 era) is never going to be the same as the Pre-COVID-19 era. Dentistry was already cited as one of the costliest professions in India, by most of the ‘poor’ (and also by some rich, as well) Indian patients; believe me, this bar is all set to go higher and further milestones are going to be breached in near future as and when we resume the regular operations of dentistry, anytime 1-3 months from now. The rampant exploitation of natural resources brought us face to face with animals that harbour these novel viruses (in this case, presumably, a bat). Eminent public health researcher Dr Peter Daszak and his team have estimated that there are as many as 5,000 coronavirus strains globally waiting to be discovered in bats. We may possibly be looking at a future where pandemics and epidemics become a part of life and health takes the centre stage in public policy and even, election campaigning, dare I say that. We will have to learn to live with the virus is the new eternal but bitter truth. I might be sounding silly here, but, health care would finally seem to take precedence over all other key issues and is slowly but surely and steadily going to get its legitimate due, very soon. As dentists and more importantly, as health care professionals we have to play our part in preparing our patients for this new reality. It was said a few years back that the World War III will not be fought with weapons; isn’t that ‘prophecy’ coming true in this COVID-19 era when thousands (rather, lacs) of people all over the world are dying for without any fault of theirs.
INTRODUCTION
The arrival of COVID-19 to the rest of the world especially Europe, which later became an epicentre of the pandemic, was not unexpected of it, having originated in Wuhan, China, Asia in late 2019. The speed of reaction and type of response to this disease around the world has been very variable according to different healthcare systems, economies and political ideologies. The local government of Wuhan did not immediately recognize the significance of the new SARS-like (Severe Acute Respiratory Syndrome) disease reported by Dr Li Wenliang, but after some initial delay, the central government of China engaged in a rapid draconian response that worked and slowed down the explosion of COVID-19 cases. Measures included lockdowns and forced quarantines on an extraordinary scale. Collection of mobile phone location data and use of facial recognition technology to track people's movements can’t readily be replicated in other countries as many would prioritize individual rights over this level of surveillance, especially in Europe; such is the story of this new materialistic world today.
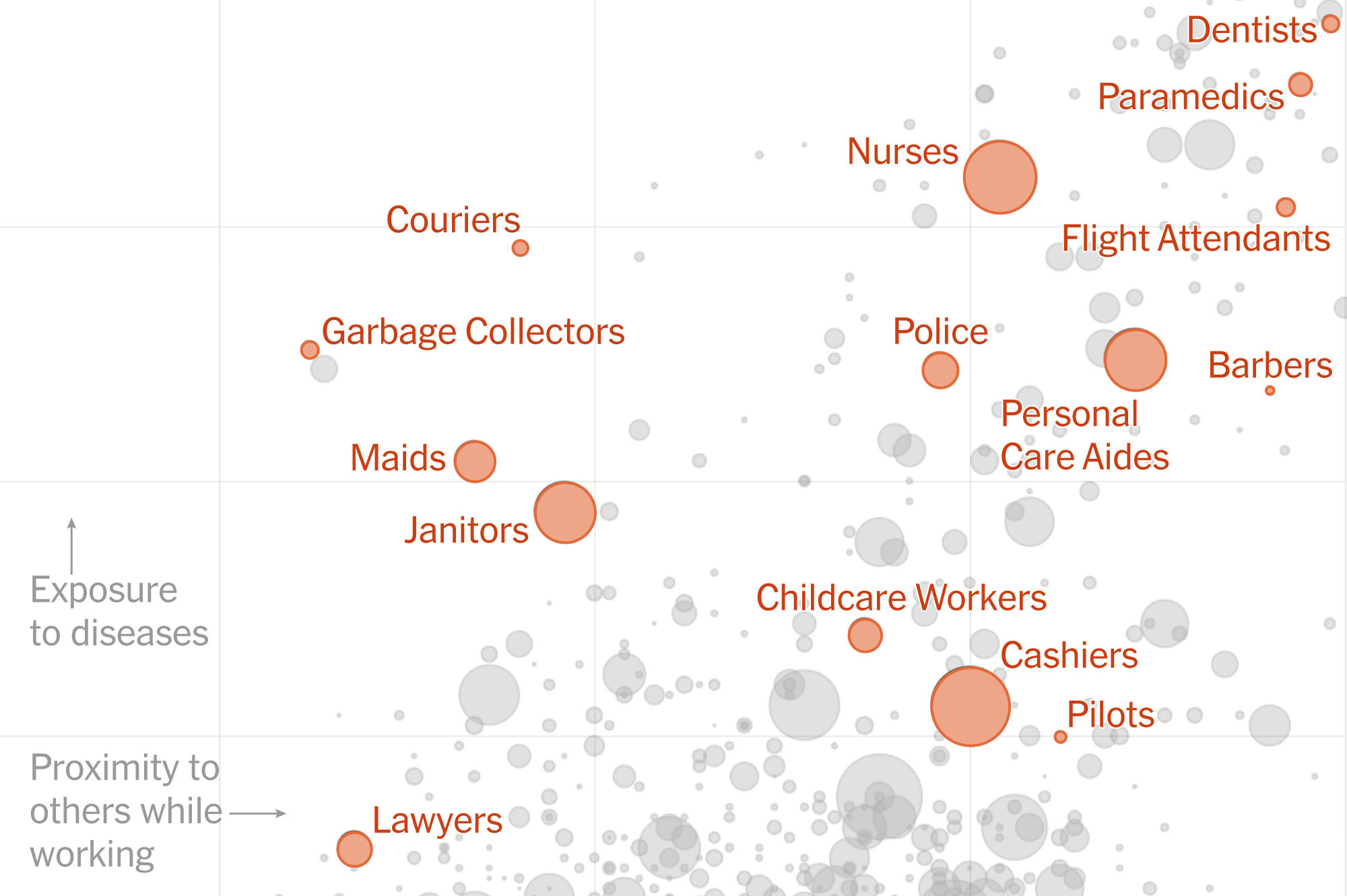
The workers who face the greatest coronavirus risk - The New York Times (15th March 2020)
China also advised that all healthcare workers use personal protective equipment (PPE), similar to that previously reserved for extremely infectious pathogens such as plague and cholera. Routine dental care was suspended in January 2020 and three months later, it is starting to get back to normal over there. Emergency dental care was provided with advice on strict personal protection and measures to reduce and avoid the production of droplets and aerosols, use of high-volume aspiration as had been recommended during the earlier SARS outbreak. The New York Times reminded the world that dentistry had the most risk of any profession in every aspect in relation to Covid-19 exposure.
However, how much risk to dental care professionals is acceptable during the COVID-19 pandemic?
The NHS initially advised that general dental care should continue unless patients had symptoms or close contact history and to use routine PPE. This supposes that patients are not infectious, if asymptomatic.
Really?
REVIEW
Let us talk of the present circumstances of COVID-19 and probably, the challenges of COSTING associated with it in the post-COVID-19 era, whenever the working resumes. In the post-COVID-19 era, improving personnel safety in healthcare environments through the appropriate use of Personal Protective Equipment (PPE) would be most likely mandatory for every dentist all over the world, especially India. Meeting such a goal would also increase adopting enhanced patient safety measures. PPE like body cover-alls, gloves, gowns, goggles and face masks as well as diagnostic and surgical products have been produced mainly by big suppliers in China. Every country is facing a shortage of equipment and the manufacturing has started in every country itself including India, reducing the dependence on China and of course, it does involve cost-cutting along with quality monitoring as well. We all are very familiar in dentistry with the principle of universal precautions for cross-infection control based on an understanding that we may not know whether a patient has the potential for disease transmission or not. As more advanced PPE is advocated for healthcare professionals caring for COVID-19 patients, then should this level of protection be used for all patients, if the transmission can occur from asymptomatic patients as mentioned above? As the in-charge of our set-up or CEO dentists, we will have to mandatorily provide for appropriate PPE for ourselves and our employees/staff (whatever the GSM requirements finally get settled and approved) and ensure that PPE is either disposable or if reusable (highly unlikely for COVID-19) are properly cleaned, laundered, autoclaved and stored (they are usually for other diseases). The compliance concerning PPE is often dependent on personal preferences. However, increased comfort (better fit, ergonomics, fewer allergies and body temperature regulation) usually translate into higher levels of compliance but at present, the comfort is directly equitable to the cost in India for those being manufactured here. We are having PPE kits from INR 100 (IIT Kanpur) to INR 5000 (imported ones from Europe / American subcontinent) with about 10 options in between this price range and they are supposed to be disposable after 1 patient as per the guidelines available now. An ideal or some sort of comfortable PPE kit is in the range of Rs. 800 (Indian make) which means minimum one for you and one for your assistant and if you are fond of 6-handed dentistry, two for your assistants. As per reports or studies coming in, the PPE kit has to be one for each patient and disposed of after that. Just assume a patient coming in for a restoration (filling) for which you earlier charged Rs. 1000 (suppose as an example). Add up the bare minimum cost of 2 PPE’s of you and your assistant to the procedure.
Won’t the landing cost of one simple restoration zoom up to around Rs. 3000?
Would it be feasible and practical?
If the option is between choosing between your lives and saving some money, what will you choose?
We all know the answer to it, whether we want to accept it or not?
All this and many more such aspects will add up the cost of doing dentistry in the post-COVID-19 era.
The escalating cost usually leads to an inverse care law.
Otherwise also speaking, before the pre-COVID-19 catastrophe, general dental practitioners believed that cost depends on the experience of the dentist too apart from lab work. If we talk of the high cost of dental care vis-à-vis patient demands, patients in today’s times (before COVID-19) were always looking for a ‘facility providing’ clinic, thus, the initial costs of setting up a clinic shot up as the exterior also needed to be done with along with the interior and of course, providing quality work which anyways is the prime requisite. Most of our medical colleagues have just got the bench and chairs in their clinic for the patients but when it comes to dentistry, patient expectations change quite a lot. In India, dental colleagues opt for urban centres because of the strong reasons of return over investment. The disparity in the economic status forces the budding doctors to opt for a sector where they are highly paid and thus, they don’t opt for rural services making it suffer a lot but on the flip side, adding to mushrooming of the clinics in urban areas. Let us just assume, these added costs in addition to an already expensive dentistry sojourn (before COVID-19), now, in the post-COVID-19 scenario. A calculation of value is an important and often required element of dental practice transitions. Calculation and management of the costs and expenses relating to clinic (business) overheads, especially when done on a monthly basis are one of the most important tools for success in any dental practice. The 4 most common reasons that dentists don’t take time out to determine the percentage of their clinic’s overhead costs and expenses include the following:
The common Indian habit of procrastination
Just too lazy
Don’t have the needed acumen to calculate the same
Simply, too busy to invest time in such activity.
Most of the Indian dentists fall into the last category whether actually busy or not. In light of the myriad of tasks and duties that must be completed on a given day, many dentists feel they don’t have enough time to calculate overheads on a regular basis. However, the ability to calculate and exert control over monthly overhead costs is vital to the continued success of any dental practice. Therefore, it is imperative that each dentist develops an effective plan which enables them to track their monthly expenses. If this is done, the clinic’s overheads can easily be tabulated. The one aspect which will surely come in handy after calculating monthly costs and expenses and determining the total monthly overhead is that many dentists will have to lower their useless expenses.
The commonest business principle which is followed otherwise in business circles to decrease overhead is to increase the production by working more hours, improving scheduling or by increasing selling price (fees, in our case). Sadly, this principle of working more hours defies logic as per the 80-20 Pareto principle.
Genuinely speaking, the first step is to examine each category of expense and to compare how it sits when seen against the ideal. Let us presume a scenario, where we start promoting our clinic and are having an increased footfall in going in lines with the above mentioned, the commonly followed business principle. When we check more new patients generally, that would result in us; allocating and spending lesser time with each patient at their initial visit and by doing that, we are either sacrificing presenting them with complete and thorough treatment options or overwhelming the new patient with rushed information digest. The most likely result in such a scenario is fewer turn-ups of the patients for actual treatment (saying a Yes) or simply saying, a poor conversion ratio. This is also known as the "roller-blading" method of dentistry which may temporarily result in higher production but does have the perennial side-effects of high overheads, fatigue, poor health and unhappiness in your personal life and to an extent clinical practice life also as and when you try understanding the numbers. If as a dentist, we don’t have good dental lab bills (that figure can vary between 30-80% for success of the gross turn over, depending on the speciality offered), we must firmly accept that we are not presenting the ideal dentistry to our patient. So, by not resorting to the latter, we are hurting our own production (talking in the business lingo) and the worst of all, not providing patients with the best treatment options possible. The same scenario goes true for cosmetic dentistry options as well. For us, as a business entrepreneur or a dentalpreneur, there are many such kinds of questions that keep us rolling in the bed and even sometimes, awake at night. Fortunately for us, we do have the requisite means to calculate the same and don’t have to go just on our gut feeling. Once we learn to apply some business principles to our decisions on fees, profitability, overhead and most useful of all, the return on investment for investments done in the clinic, believe me, life can be as rosy as you can expect. We have to take into account all such aspects in the post-COVID-19 era as regards to newer investments as our running costs are going to grow manifold and the incoming cash collection won’t be coming at the same pace and volume as before due to the decreased purchase power of the patients because of a strong recession in the economy. Every such decision of investment in the clinic; be it, the buying of new equipment or an expensive material has now to be backed by scientific logic, a basic understanding of your figures and numbers and calculation of costs. If we don’t do this, all the above has potential for the costs to be snowballed into an enhanced effect.
How? Let us see further.
In post-COVID –19 era, the word ‘Life’ as such per se is going to change its meaning, forever and social distancing is going to be the new norm. Our profession, Dentistry is also not going to be left untouched from the same and we have to anticipate and expect inflation in expenses and accordingly, we have to escalate charges in our dental clinics. As each day is passing in this lockdown, new SOP’s (Standard Operating Protocol) are coming up from many of the stalwarts of the business. The way I can envision it, many things are going to change forever in dentistry, whether or not all dentists wish to adopt the same or not. I strongly believe, the economics is going to change drastically for most of the dentists and accordingly, the cost factor will have to take into account for the same. We surely will need to go back to our basics of knowing our figures and numbers and that would also mean eliminating the unwanted expenses when the more prudent ones start taking the precedence. We all will be having less working man-hours now effectively, considering the addition of intricacies of donning and doffing the PPE suits every now and then. So, the planning would have to imperatively rotate around the aspect of treating less but charging more vis-à-vis the aspect that the input expenses are now all set to go higher.
Let me first deal a bit on increased charging. How are we going to achieve that?
Dr Bhavdeep Singh Ahuja graduated in 1998 from Punjabi University, Patiala. He has specialized in Implants from BioHorizons Inc. USA in 2004-05 & in Advanced Course from LACE-ICOI, USA in 2006. Apart from Dentistry, he holds a Triple M.B.A. in Hospital Management, Finance/Human Resources (dual) & Marketing from three premier Institutes/Universities of India viz. the IIMM Pune, IGNOU Delhi & Annamalai University, Chennai respectively. He also holds Post Graduate Diploma’s in Medical Law & Ethics (NLSIU - Premier LAW School of India), Clinical Research, Cyber Law, IPR's (Intellectual Property Rights), Disaster Management, Financial Management, Bioinformatics amongst many more from different Universities. He is a Certified Health Care Waste Manager from IGNOU & is qualified in Consumer Law as well. He is an academically oriented dentist & has more than 75 Original Scientific Publications to his credit in many International & National journals. He lectures all over India extensively on the topics of Practice Management, Medical Law, Ethics and Consent and Finance for Dentists and he is writing a series on all these topics in multiple journals simultaneously. He has been the Past Editor-in-Chief, L.E.D. E-Journal & PAGE 3 OLA-D E-Newsletter, the twin Publications of IDA Ludhiana Branch. Presently, he is into his 21st year of Clinical Private Practice in Ludhiana, Punjab.
COVID-19 is having an unprecedented impact on the global economy, including that of the dental industry. Most dental clinics are shut and a few are offering...
COVID-19 is having an unprecedented impact on the global economy, including that of the dental industry. Most dental clinics are shut and a few are offering...
COVID-19 is having an unprecedented impact on the global economy, including that of the dental industry. Most dental clinics are shut and a few are offering...
COVID-19 is having an unprecedented impact on the global economy, including that of the dental industry. Most dental clinics are shut and a few are offering...
Artificial Intelligence (AI) has been pivotal in refining diagnostic accuracy and revolutionizing care. Of all the applications that AI can provide us, ...
New Delhi: The two day SYFAC programme organized by LifeCare Devices Private Limited during a cold weekend of 9-10 December 2017 was attended by over 80 ...
Rapid Antigen Tests are an easy and economical option for dentists to use in their clinics to identify the potential Covid-19 spreaders visiting their ...
Dental litigation is on the rise in India, placing growing legal and ethical demands on practitioners. This article explores the key factors driving this ...
Education
Live webinar Tue. 4 August 2026 5:30 am IST (New Delhi)
Tooth decay remains the most widespread chronic health condition globally, affecting billions of people. While cavities are largely preventable and ...
MUMBAI, India: Can clinicians identify patients at higher risk of implant complications before surgery? Can understanding the patient’s immune response ...
Implant dentistry has evolved significantly through advances in implant design, surface technology and digital workflows. However, the process of osteotomy ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE














")




")
")
")
")




















Excellent analysis.